The (un)fair allocation of scarce vaccines and how math can provide a solution
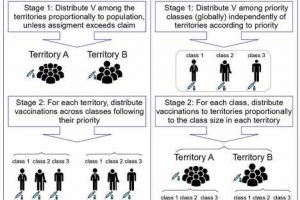
 (left) shows the two stages of the Territorial Allocation protocol, which captures the essential features of those actually used for COVID-19. (B) (right) shows the two stages of the Priority-Equality protocol, which we identify in this work as the only one satisfying fundamental ethical principles. Credit: Frontiers in Public Health (2022). DOI: 10.3389/fpubh.2022.986776")
Remember when COVID-19 vaccines first became available? After many months of lockdowns and increasing casualty rates, people across the planet were allowed to exhale a collective sigh of relief. However, as is always the case when new vaccines are developed, there were not enough doses for all who wanted them. Rationing had to be imposed.
Unfortunately, the rationing procedures violated elementary ethical principles, which might have led to some elderly and at-risk patients being neglected while younger, healthier citizens were already vaccinated.
How did it go wrong? Vaccine acquisition and allocation across the world was as centralized as possible, to avoid a free-for-all race where individual countries and regions tried to secure vaccines for its citizens to the detriment of others. The World Health Organization and other organizations supported a multi-country initiative called COVAX, the EU acted on behalf of all its member states, and large countries like the US took charge of distribution among their constituent states.
What these organizations apparently forgot was that first, there is a large debate in medical ethics on what constitutes a fair and ethical allocation of vaccines, and second, there are scientists (mathematicians and economists) who study the allocation of scarce resources.
Priority and equality
In the case of vaccines, two ethical principles are most important. First, there should be priorities. To avoid collapse, medical personnel should be immunized first. The elderly and those at higher risk should be inoculated before others, and so on. This principle, called “prioritizing according to needs,” requires that the priority classes (as decided by the competent medical authorities) should be respected, and immunization of a priority class should not start until those in previous priority classes have been inoculated.
Second, everybody within a given priority class should be treated equally. This principle, called “treating equal people equally,” requires that people with the same priority have the same chance of receiving the vaccine, irrespective of irrelevant factors as, say, in which country or state within the alliance they might reside.
My new article in Frontiers in Public Health, compiled with J. García-Segarra and M. Ginés-Vilar, shows that the allocation of COVID-19 vaccines violated those principles, and not only in theory. For instance, the differences in vaccination rates for given priority classes in EU countries was astonishing. By the 12th week of 2021, the percentage of vaccinated healthcare workers (the highest priority class) was as high as 71.5% in Romania or 66.9% in Estonia and as low as 36.8% in Denmark or 21.5% in Iceland.
That is ignoring special cases as Bulgaria, where vaccine hesitancy kept the rate even lower, or Hungary, which secured additional vaccines on its own. Ten weeks later, some EU-countries such as Spain and Belgium had received enough vaccines for all healthcare workers and all those aged 70 or older, while Denmark, France, and Greece only had received enough to immunize those older than 80.
Such differences did not go unnoticed by the population either, as shown by a number of anecdotal cases of individuals crossing national boundaries to receive their vaccines earlier.
Why did this happen? The allocation protocols used by COVAX or the EU followed political criteria, but ignored scientific and ethical ones. Essentially, they divided the stock of available doses in lots proportional to the population of the member territories, and shipped [the] lots to them with instructions to immunize people according to priorities. The problem is that the proportion of the priority classes is different in different territories.
Suppose two territories have the same population, so they will receive the same number of vaccines, say 500,000. The first territory has a relatively young population, with just 300,000 healthcare workers and elderly citizens, and hence will immunize all of them and start immunizing those with lower priority. The second territory has a relatively old population, with 700,000 healthcare workers and elderly people.
Hence it will not even have enough vaccines to immunize all the elder citizens. Even though both territories receive vaccine doses from the same alliance, 200,000 elder citizens in the second might be dying from lack of vaccines while 200,000 younger, healthier citizens are already vaccinated in the first territory.
How to allocate scarce vaccines
Did this need to happen? No. The problem can be solved using techniques from the mathematical social sciences. In our article, we have shown mathematically that there is one and only one way to allocate vaccines, ensuring that in multi-territory vaccine alliances, priority classes are respected and people within given priority classes are treated equally. The procedure, the “Priority-Equality Protocol,” is a bit more complex than the ones that were used for the case of COVID-19, but not exceedingly so.
First, one adds up the size of the priority classes across territories, e.g., how many healthcare workers, elderly, etc., are there in the entire EU.
Second, the stock of vaccines is allocated to the priority classes (not to the countries) proportionally to their size.
Last, vaccinations are shipped to countries earmarked for the priority classes, proportional to the size of those classes relative to the corresponding ones in other countries. For instance, the two territories in the example above would have received 300,000 and 700,000 vaccines, respectively, corresponding to the number of healthcare workers and elder citizens.
Of course, administrative and logistical problems remain. However, what the math says is that there is no other method respecting both ethical principles mentioned above. We all hope there will not be a next time, but if there is, we now know better: The Priority-Equality Protocol is ready to use and any other protocol would (now knowingly) be a violation of elementary ethical principles.
More information:
Carlos Alós-Ferrer et al, Ethical allocation of scarce vaccine doses: The Priority-Equality protocol, Frontiers in Public Health (2022). DOI: 10.3389/fpubh.2022.986776
Journal information:
Frontiers in Public Health
Source: Read Full Article