effexor withdrawal severe anxiety
. DOI: 10.1101/2022.12.16.22283585")
Three years into the COVID-19 pandemic, new variant outbreaks continue to fuel economic disruptions and hospitalizations across the globe. Effective therapies remain unavailable in much of the world, vermox suspension dosis unica and circulating variants have rendered monoclonal antibody treatments ineffective. But a new analysis shows how convalescent plasma can be used as an effective and low-cost treatment both during the COVID-19 pandemic and in the inevitable pandemics of the future.
In a study published on Clinical Infectious Diseases, an international team of researchers analyzed clinical data and concluded that among outpatients with COVID-19, antibodies to SARS-CoV-2 given early and in high dose reduced the risk of hospitalization.
“If the results of this meta-analysis had somehow been available in March of 2020, then I am certain that millions of lives would have been saved around the world,” said study author Dr. Adam C. Levine, a professor of emergency medicine at Brown University’s Warren Alpert Medical School.
While several other early treatments for COVID-19 have had similar results, including antivirals like Paxlovid and monoclonal antibodies, only convalescent plasma, the researchers concluded, is likely to be both available and affordable for the majority of the world’s population both now and early in the next viral pandemic.
“These findings will be helpful for this pandemic, especially in places like China, India and other parts of the world that lack access to antiviral medications like Paxlovid,” Levine said. “And because it provides information on how to more effectively use convalescent plasma as a therapy, this will be even more helpful in the next pandemic. This study is essentially a roadmap for how to do this right the next time.”
Blood plasma from people who have recovered from COVID-19 and contains antibodies against SARS-CoV-2 was used as a treatment early in the pandemic, Levine said—months before monoclonal antibody treatment or vaccines became available, and more than a year before an effective oral drug therapy was clinically available.
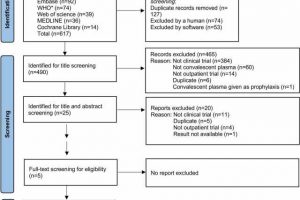
Although convalescent plasma seemed promising, outpatient research was limited, and studies that did exist showed mixed results. One problem was that most studies were conducted in patients already hospitalized with COVID-19, Levine said, largely due to the convenience of conducting research with this population. The objective in the new study was to review all available randomized controlled trials of convalescent plasma in non-hospitalized adults with COVID-19 to determine whether early treatment can reduce the risk of hospitalization.
The analysis included data from five studies conducted in four countries, including Argentina, the Netherlands, Spain, and two in the United States. Levine previously supervised enrollment at Rhode Island Hospital in a clinical trial led by Johns Hopkins Medicine and Johns Hopkins Bloomberg School of Public Health.
Across the five studies, a total of 2,620 adult patients had received transfusions of convalescent plasma from January 2020 to September 2022. The researchers conducted an individual participant data meta-analysis to assess how the transfusion timing and dose impacted the patient’s risk of hospitalization during the 28 days after infection.
In their analysis, the researchers found that 160 (12.2%) of 1,315 control patients were hospitalized compared with 111 (8.5%) of 1,305 patients treated with COVID-19 convalescent plasma—30% fewer hospitalizations.
Notably, the strongest effects were seen in patients treated both early in the illness and with plasma with high levels of antibodies. In these patients, the reduction in hospitalization was over 50%.
For future pandemics, the goal is to use plasma from donors who have high levels of antibodies, said corresponding study author Dr. David J. Sullivan, a professor of molecular microbiology and immunology at Johns Hopkins Bloomberg School of Public Health and School of Medicine. “This research suggests that we have been underdosing convalescent plasma for many previous pathogens, which impacts effectiveness,” Sullivan said. “It bears repeating: Early and high levels of antibodies increased the beneficial efficacy.”
Levine explained that because convalescent plasma was the only treatment available at the beginning of the pandemic, it was used widely—and often incorrectly, on hospitalized patients who were already experiencing severe symptoms late in the course of COVID-19. Those symptoms were due to a ramped-up immune response to the virus, not the virus itself.
“By the time the patient was at the point where they’d reached the inflammatory phase that caused severe symptoms, it was too late for treatments like convalescent plasma or even monoclonal antibodies to work,” he said.
What is now known is that convalescent plasma works best when given early in the course of illness. That’s when it can neutralize the virus and get ahead of the body mounting an intense immune response, thereby preventing hospitalization and death, Levine said.
The five drug treatment trials in the analysis took place at a variety of global health care sites, he noted, including nursing homes, outpatient clinics and emergency departments. The diversity across the studies is a sign that the data is likely generalizable to many other types of populations and settings around the world, said Levine, who also directs the Center for Human Rights and Humanitarian Studies at the Watson Institute for International and Public Affairs at Brown.
Levine cited another recently published study in JAMA Network Open that showed that convalescent plasma is effective in reducing mortality in immunocompromised patients. This new meta-analysis provides evidence that convalescent plasma can also be effective in the larger population of adults who are not immunocompromised.
The U.S. Food and Drug Administration allowed early convalescent plasma use in December 2021 for those patients with COVID-19 who were also immunocompromised, but not yet for patients with COVID-19 who are not immunocompromised. The authors said they hope the new study will push the FDA, and other countries around the world, to make early treatment with COVID-19 convalescent plasma available to a much larger group of patients at risk for hospitalization.
A treatment that evolves with the pandemic
The findings come at a time when monoclonal antibodies, the most commonly used treatment for COVID-19, have been shown to be ineffective against new variants of the virus. In November, the FDA revoked emergency authorization of the last monoclonal antibody treatment because it wasn’t expected to have much of an effect against Omicron sub-variants.
In contrast to monoclonal antibody therapies, Levine said, convalescent plasma donated by patients who have recovered from the virus is a treatment that evolves with the pandemic. Because it has antibodies that attach to multiple different parts of the virus, there are still opportunities to attach to a receptor even after the virus mutates and morphs some of its receptors. It’s also less expensive to produce than pharmaceutical antivirals.
In the first year of the pandemic, Levine said, before the development of vaccines and effective treatments, researchers tried many treatment strategies in order to quickly find something that worked to save lives.
“When the next big pandemic hits, we’re going to be in a very similar situation,” Levine said. “Yet at least next time, we’ll have research like this to inform our strategy.”
More information:
David J Sullivan et al, COVID-19 Convalescent Plasma Outpatient Therapy to Prevent Outpatient Hospitalization: A Meta-analysis of Individual Participant Data From Five Randomized Trials, Clinical Infectious Diseases (2023). DOI: 10.1093/cid/ciad088. academic.oup.com/cid/advance-a … /cid/ciad088/7048396
Jonathon W. Senefeld et al, COVID-19 Convalescent Plasma for the Treatment of Immunocompromised Patients: A Systematic Review and Meta-analysis, JAMA Network Open (2023). DOI: 10.1001/jamanetworkopen.2022.50647
Journal information:
Clinical Infectious Diseases
,
JAMA Network Open
Source: Read Full Article