Blood thinners may improve survival among hospitalized COVID-19 patients

Treating hospitalized COVID-19 patients with anticoagulants—blood thinners that slow down clotting—may improve their chances of survival, researchers from the Mount Sinai COVID Informatics Center report. The study, published in the May 6 issue of the Journal of the American College of Cardiology, could provide new insight on how to treat and manage coronavirus patients once they are admitted to the hospital.
The study found that hospitalized COVID-19 patients treated with anticoagulants had improved outcomes both in and out of the intensive care unit setting. The research also showed that the difference in bleeding events among patients treated with and without anticoagulants was not significant. The Mount Sinai researchers say their work outlines an important therapeutic pathway for COVID-19 patients.
“This research demonstrates anticoagulants taken orally, subcutaneously, or intravenously may play a major role in caring for COVID-19 patients, and these may prevent possible deadly events associated with coronavirus, including heart attack, stroke, and pulmonary embolism,” says senior corresponding author Valentin Fuster, MD, Ph.D., Director of Mount Sinai Heart (the nation’s number six ranked hospital in Cardiology/Heart Surgery) and Physician-in-Chief of The Mount Sinai Hospital. “Using anticoagulants should be considered when patients get admitted to the ER and have tested positive for COVID-19 to possibly improve outcomes. However, each case should be evaluated an individualized basis to account for potential bleeding risk.”
The publication of this study follows recent research out of the Icahn School of Medicine at Mount Sinai that shows a large number of patients hospitalized with COVID-19 have developed high levels of life-threatening blood clots, leading to potentially deadly thromboembolic events.
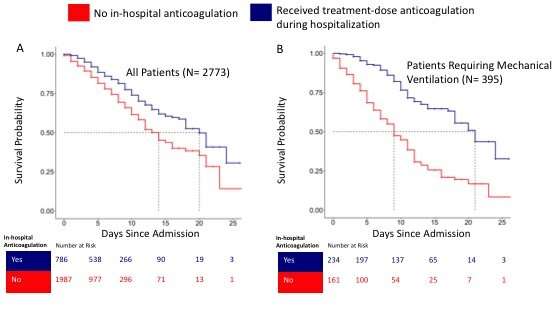
A team of investigators evaluated records of 2,773 confirmed COVID-19-positive patients admitted to five hospitals in the Mount Sinai Health System in New York City (The Mount Sinai Hospital, Mount Sinai West, Mount Sinai Morningside, Mount Sinai Queens, and Mount Sinai Brooklyn) between March 14 and April 11, 2020. They specifically looked at survival rates for patients placed on blood thinners versus those not placed on blood thinners. The researchers took certain risk factors into account before evaluating the effectiveness of anticoagulation, including age, ethnicity, pre-existing conditions, and those already on blood thinners.
Of the COVID-19 patients analyzed, 786 (28 percent) received a full-treatment dose of anticoagulants—a higher dose than what is typically given for blood clot prevention, and one that is usually given to those who already have clots or are suspected to have clots. Treatment with anticoagulants was associated with improved hospital survival among COVID-19 patients both in and out of the intensive care unit setting. Of the patients who did not survive, those on anticoagulants died after spending an average of 21 days in the hospital, compared to the non- anticoagulant patients who died after an average of 14 days in the hospital. The effect of anticoagulation had a more pronounced effect on ventilated patients—62.7 percent of intubated patients who were not treated with anticoagulants died, compared to 29.1 percent for intubated patients treated with anticoagulants. Of the intubated patients who did not survive, those with no anticoagulants died after 9 days, while those on anticoagulants died after 21 days.
All patients in the study had blood work done when they arrived at the hospital, which included measuring various inflammatory markers. The analysis of their records showed patients who received anticoagulants had higher inflammatory markers compared to patients not treated with anticoagulants. This may suggest patients with more severe illness may benefit from anticoagulants early on.
The observational study also explored the association of systemic anticoagulant treatment with bleeding events. Major bleeding was defined as 1) hemoglobin <7 g/dL and any red blood cell transfusion; 2) at least 2 units of red blood cell transfusion within 48 hours; or 3) a diagnosis code for major bleeding including intracranial hemorrhage; hematemesis; melena; peptic ulcer with hemorrhage; colon, rectal, or anal hemorrhage; hematuria; ocular hemorrhage; and acute hemorrhagic gastritis. Among those who did not receive anticoagulants, 38 (1.9 percent) patients had bleeding events, compared to 24 (3 percent) among those who received anticoagulants, p=0.2).
“We are hopeful that this report of the association of anticoagulation therapy with improved survival will be confirmed in future investigations. The astute scientists at Mount Sinai continue to analyze our data on COVID-19 patients in order to contribute to worldwide efforts to find effective treatments,” says David Reich, MD, President and Chief Operating Officer of The Mount Sinai Hospital.
“As a cardiologist who has been on service caring for COVID-19 patients for the last three weeks, I have observed an increased amount of blood clot cases among hospitalized patients, so it is critical to look at whether anticoagulants provide benefits for them,” says co-researcher Anu Lala, MD, Assistant Professor of Medicine (Cardiology) at the Icahn School of Medicine at Mount Sinai. “It’s important to note that further analysis and prospective studies are required to determine the effectiveness for widespread use of anticoagulants in hospitalized COVID-19 patients.”
Source: Read Full Article