Longer between-dose intervals for COVID-19 vaccines may significantly reduce mortality

A recent study, currently available on the medRxiv* preprint server, has shown how longer dosing intervals of vaccines against coronavirus disease (COVID-19) may be able to minimize mortality in low- and middle-income countries in the WHO European region – and significantly change our vaccination strategy.
As the COVID-19 pandemic is still having a strong global impact, it is pivotal that countries maximize the health benefits of the available vaccine supplies based on context-specific COVID-19 epidemiology, transmission dynamics, and pre-existing immunity COVID-19 vaccine immunogenicity, efficacy, and safety.

Vaccines currently on the market usually involve two doses with specific between-dose intervals, as informed by the clinical trials. More specifically, the time span between two vaccine doses is usually 3-4 weeks, although this may vary among different solutions.
Nonetheless, in practice, countries may utilize dosing intervals that are longer than recommended due to a plethora of different factors, most notably vaccine shortages, logistic constraints and administrative issues, but also comparable and potentially higher vaccine efficacy with the extended dosing interval.
To address this information gap, a research group from the London School of Hygiene & Tropical Medicine and Public Health England aimed to estimate the health impact and risk-benefit assessment of COVID-19 vaccination regarding different dosing intervals for low- and middle-income countries in Europe.
A stringent modeling approach
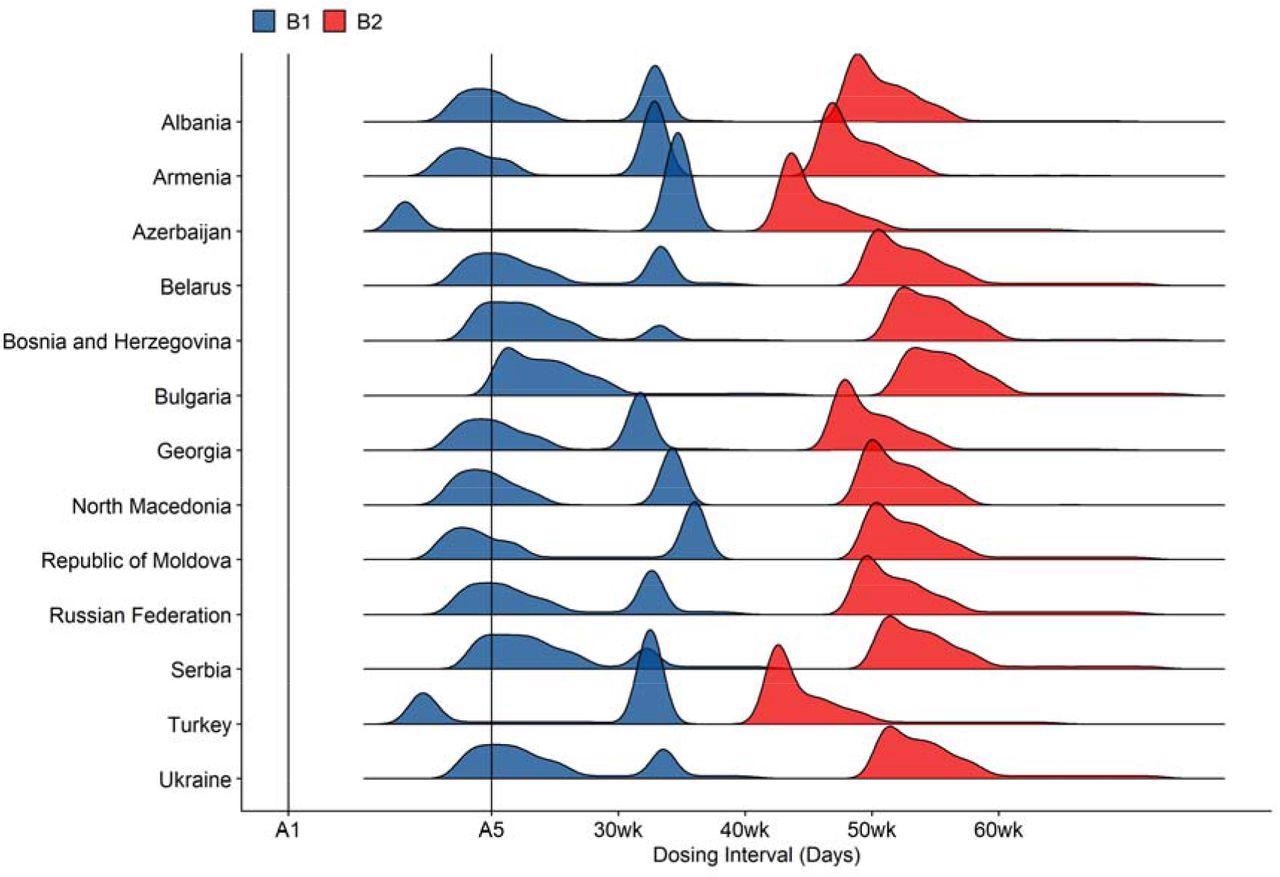
For that purpose, this research group used a dynamic transmission model that incorporated daily nationwide COVID-19 mortality in thirteen low- and middle-income countries, which are (alphabetically): Albania, Armenia, Azerbaijan, Belarus, Bosnia and Herzegovina, Bulgaria, Georgia, Republic of Moldova, Russian Federation, Serbia, North Macedonia, Turkey, and Ukraine.
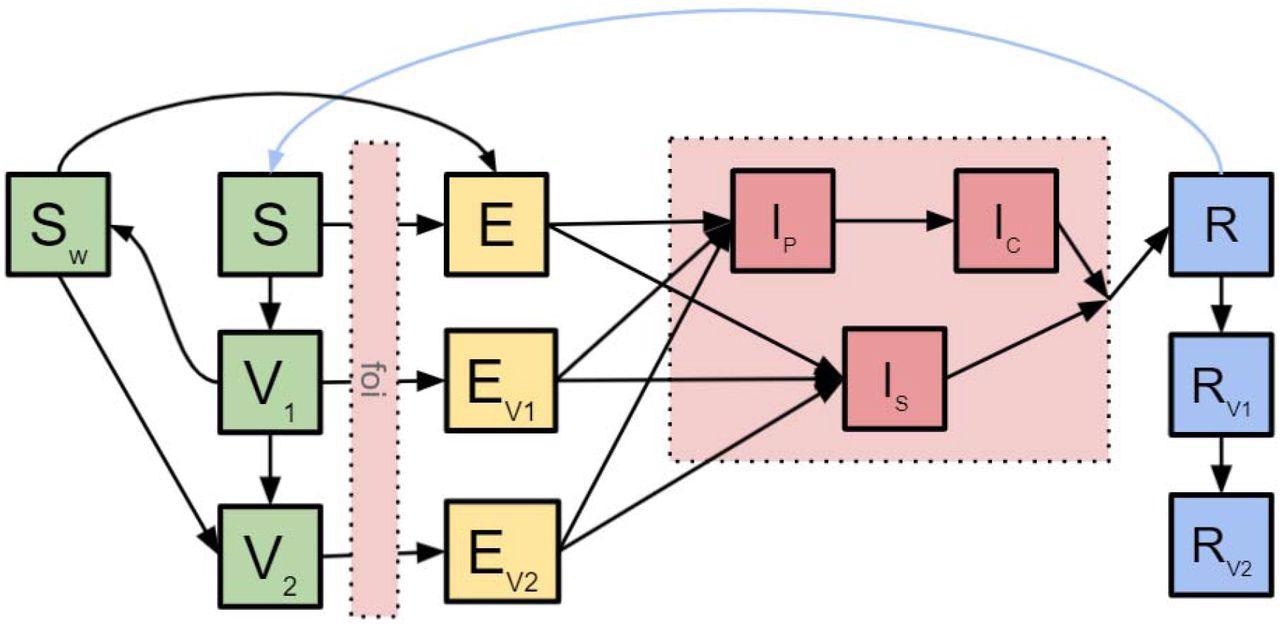
A vaccine similar to the Oxford-AstraZeneca COVID-19 (AZD1222) vaccine was used in the base case scenario, supplemented by sensitivity analyses regarding efficacies related to other COVID-19 vaccines. Furthermore, the scientists have used fixed dosing intervals at 4, 8, 12, 16, and 20 weeks and dose-specific intervals that prioritize specific doses for specific age groups.
Finally, the emergence of variants of concern has been accounted for in the model with adequate sensitivity analyses. At the same time, a risk-benefit assessment was conducted in order to quantify the trade-off between any harm caused by adverse events and health benefits after immunization procedure.
An enormous efficacy of longer dosing intervals
This study revealed that optimal strategies are, in fact, those that prioritize the first doses among adults older than 60 years of age, or those between 20-59 years of age, which was valid for 12 out of the 13 countries. More importantly, these strategies resulted in dosing intervals longer than six months, as a 4-week fixed dosing interval may give rise to 10.2% more fatal outcomes.
There was also a negative association between dosing interval and COVID-19 mortality within the investigated range. In comparison to risks, benefits were highest for strategies that included 8-12 weeks intervals, following the age-dependent rates of prevented deaths from COVID-19.
Although the researchers could not extend the modeling further into 2021 due to data availability issues, the available results point towards a sizeable efficacy of longer dosing intervals; however, the paper highlights how extraordinarily long dosing intervals should be avoided.
Benefits for societies around the world
In any case, even though dosing intervals of over six months are significantly longer than the current label recommendation for most vaccines, this approach could reduce COVID-19 mortality in low- and middle-income countries in Europe. Still, it has to be noted that certain vaccine features (such as fast waning of first doses) significantly shorten the optimal dosing intervals.
“The results we have observed are robust to different vaccine characteristics assumptions of vaccine efficacy estimates versus dosing interval relationships,” further emphasize the authors of this medRxiv paper. “Including additional outcomes and benefits for society is expected to lead to similar results,” they add.
Since countries that were included in this study have diverse demographics and age structures, contact patterns and historical outbreak experiences histories, the overall conclusions can be valuable in decision-making in low- and middle-income countries around the world.
*Important Notice
medRxiv publishes preliminary scientific reports that are not peer-reviewed and, therefore, should not be regarded as conclusive, guide clinical practice/health-related behavior, or treated as established information.
- Liu, Y. et al. (2021). Dosing interval strategies for two-dose COVID-19 vaccination in 13 low- and middle-income countries of Europe: health impact modelling and benefit-risk analysis, medRxiv, https://doi.org/10.1101/2021.11.27.21266930, https://www.medrxiv.org/content/10.1101/2021.11.27.21266930v1
Posted in: Medical Research News | Disease/Infection News | Pharmaceutical News
Tags: Coronavirus, Coronavirus Disease COVID-19, Efficacy, Epidemiology, Hygiene, immunity, Immunization, Medicine, Mortality, Pandemic, Public Health, Research, SARS, SARS-CoV-2, Vaccine

Written by
Dr. Tomislav Meštrović
Dr. Tomislav Meštrović is a medical doctor (MD) with a Ph.D. in biomedical and health sciences, specialist in the field of clinical microbiology, and an Assistant Professor at Croatia's youngest university – University North. In addition to his interest in clinical, research and lecturing activities, his immense passion for medical writing and scientific communication goes back to his student days. He enjoys contributing back to the community. In his spare time, Tomislav is a movie buff and an avid traveler.
Source: Read Full Article