fenofibrate sexual side effects
<img class="aligncenter" src="https://scx1.b-cdn.net/csz/news/800a/2023/review-strengthens-evi.jpg"
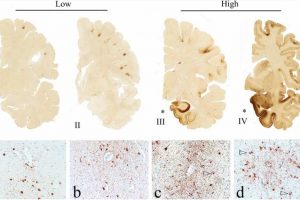
alt="Review strengthens evidence that repetitive head impacts can cause CTE"
title="The pathognomonic lesion of CTE and the staging schemes of pathological severity (adapted with permission from [83]). Representative images of p-tau pathology at Low and High chronic traumatic encephalopathy (CTE) pathological stage using the abbreviated staging scheme recommended by the second NINDS/NIBIB consensus panel (low–high) [11] and the McKee staging scheme (I–IV) [4, 79]. Low CTE is characterized by p-tau pathology restricted to focal cortical lesions. High CTE shows widespread p-tau pathology in the medial temporal lobe structures and diencephalon in addition to focal cortical lesions. McKee Stage I CTE is characterized by one or two isolated CTE lesions at the depths of the cortical sulci. In stage II, three or more cortical CTE lesions are found. In stage III CTE, there are multiple CTE lesions and diffuse NFTs in the medial temporal lobe. In stage IV CTE, CTE lesions and NFTs are widely distributed throughout the cerebral cortex, diencephalon, and brainstem. Top row: hemispheric 50-µm tissue sections immunostained with CP-13, directed against phosphoserine 202 of tau (courtesy of Peter Davies, Ph.D., nateglinide versus repaglinide for type 2 diabetes mellitus in china Feinstein Institute for Medical Research; 1:200); positive p-tau immunostaining appears dark brown. Bottom row: 10-µm paraffin-embedded tissue sections immunostained for phosphorylated tau (AT8) (Pierce Endogen). Positive p-tau immunostaining appears dark red, hematoxylin counterstain. I A 26-year-old former college football player with stage I CTE (Low). Two perivascular p-tau CTE lesions are evident at the sulcal depths of the frontal cortex; there is no neurofibrillary degeneration in the medial temporal lobe. II A 49-year-old former NFL player with stage II CTE (Low). There are multiple perivascular p-tau CTE lesions at depths of sulci of the frontal cortex; there is no neurofibrillary degeneration in the amygdala or entorhinal cortex. III A 53-year-old former NFL player with stage III CTE (High). There are multiple CTE lesions in the frontal cortex and insula; there is diffuse neurofibrillary degeneration of hippocampus and entorhinal cortex (asterisk). IV A 62-year-old former NFL player with stage IV CTE (High). There are multiple CTE lesions in the cerebral cortex with widespread neurofibrillary degeneration. There is also extensive neurofibrillary degeneration of the amygdala and entorhinal cortex (asterisk). a Pathognomonic CTE lesion in stage I CTE. AT8 immunopositive neurofibrillary tangles, dot-like and threadlike neurites encircle a small blood vessel. b Pathognomonic CTE lesion in stage II CTE. A cluster of AT8 immunopositive neurofibrillary tangles and dense dot-like neurites surround several small blood vessels, c pathognomonic CTE lesion in stage III CTE. A large collection of AT8 immunopositive neurofibrillary tangles and dense dot-like neurites enclose several small blood vessels. With increasing age, AT8 immunoreactive astrocytes are increasingly evident within the pathognomonic lesion (open triangle). d Pathognomonic CTE lesion in stage IV CTE. A large accumulation of AT8 immunopositive neurofibrillary tangles, most of them ghost tangles, encompass several small blood vessels. With increasing age, AT8 immunoreactive astrocytes are increasingly prominent (open triangles) and there may be evidence of neuronal loss. a–d All magnification × 200. P-tau phosphorylated tau, CTE chronic traumatic encephalopathy, NFL National Football League. Credit: Acta Neuropathologica (2023). DOI: 10.1007/s00401-023-02540-w” width=”800″ height=”489″>
Source: Read Full Article